- - - - - -Last updated on Tuesday, February 8, 2005
- - - - - -Last updated on Tuesday, February 8, 2005
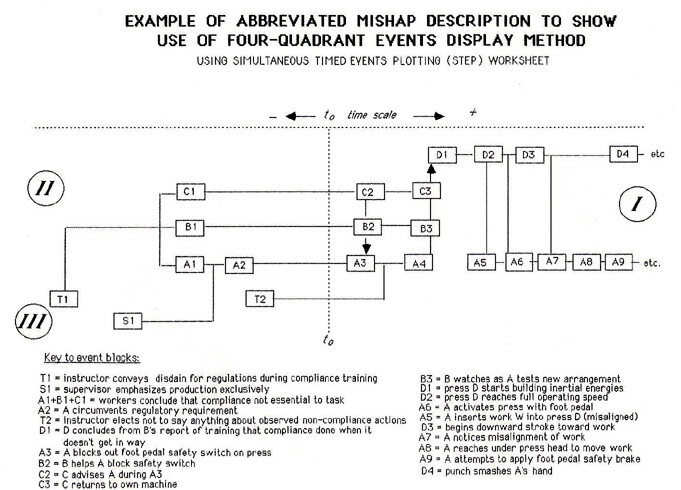
INTRODUCTIONIn 2005, while preparing the 1987 paper for posting on the Archives web site, I found in the old file folder several additional illustrations that were prepared while the 1987 paper was being developed. These graphics illustrate the development of the conceptual framework for capturing and organizing specific behaviors of individuals with a role in accident and incident processes, to determine human performance in accidents and incidents. The need for the framework and its application are described in the 1987 paper. Each illustration is followed by commentary about its origins and development. Software supporting the framework and its application has now been developed. THE BASIC FRAMEWORK
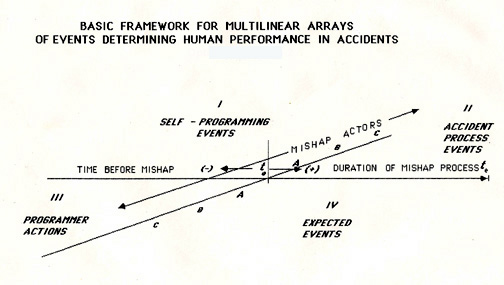
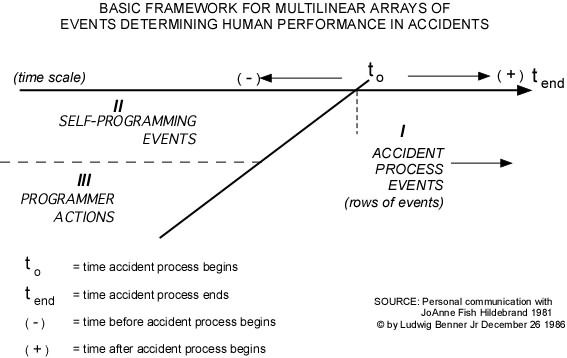 Early investigative efforts to identify and describe why things happened as they did during accidents led to what influenced individuals to do what they did during accidents and incidents. That quest resulted in, among other findings, my differentiating habituated responses from adaptive responses when individuals were trying to cope in real time with events that were occurring around them and to them. At the time, I was also experimenting with data organization and display efforts to help with the development of descriptions and explanations of accidents I was investigating. A personal experience that further spurred the development of this technique occurred during an open NTSB meeting. A truck driver who was trying to disconnect a battery wire in his wrecked gasoline tank-trailer vehicle died in a fire that was ignited by his actions. Knowing from the investigation that the driver died because he did what he was trained to do, it was discouraging to hear a Member observe "That was a dumb thing to do" while discussing the driver's actions. I was frustrated that I had not demonstrated clearly enough so anyone could understand how the driver's "habituated" behavior was produced by his prior training. Narrative descriptions obviously were not getting the job done. I was trying to respond to that challenge when I started exploring the displays reported in the 1987 paper. While pursuing attempts to identify what produced habituated responses, or what actions or experiences "programmed" the observed habituated responses, I had discussions with a few interested colleagues who were kind enough to listen to what I was trying to explain. This first illustration resulted from a challenge during a discussion with a friend who suggested that it was difficult to comprehend what I was talking about. So these illustrations were developed, leading, in part, to the illustrations and content of the 1987 paper. The first illustration depicts the two kinds of "programming" behaviors that influence subsequent behaviors during an accident or incident process: external programming and self-programming. To program is to cause or absorb or incorporate automatic responses. attitudes or the like. in other words condition people or objects to behave in a particular way. Programming behaviors, for the purposes of assessing human performance, are the actions by people, objects or energies that are observed by an individual, and that influence subsequent actions by the individual, producing "habituated" responsive behaviors. External programming results from actions by other people or objects, and self-programming results from personal experiences from which individuals draw conclusions about future behaviors and thenact on those conclusions. The programming actions can be objectively identified in concrete terms by identifying the actions that "conditioned" specific subsequent actions. Identifying these specific programming actions should be a major objective for incident investigators. In the MES system, such actions are identified as "change makers." It must be noted that programming actions do not usually, by themselves, result in process deviations or excursions, but rather, in combination with other changes, they require identification to fully understand why people or objects did what they did. Figure 5 at the end of this addendum offers examples of "programming" behaviors which exerted such an influence on subsequent actions. COMPARING ACTUAL VS EXPECTED ACTIONS |